In Vitro maturation (IVM), the concept includes the idea when the eggs are removed from the ovaries of the woman body and transfer them into the laboratory for two or three for being fertilized. This procedure mainly applies when the causes of infertility find out in the male factor only not in the female factor. When the eggs are mature so that is fertilized with partner’s sperm or donor sperm. This is the definition of the IVM now look at the meaning of the IVF means when the patient is not able to conceive the child so they attempt the procedure of IVF in virto fertilization means when are eggs and the sperm of the couple get fertilization in the labotray dish when the embryo get moves so the it transfer in the uterus of the women where the pregnancy implanted and it grow day by grow. IVF is the natural procedure and the different is in the IVF procedure the fertilization takes part out of the body and in then normal pregnancy it takes part in the human body. The medical science is touching the sky and the best example is the more then IVF there are other fertility potions as well and the best example; IVM.
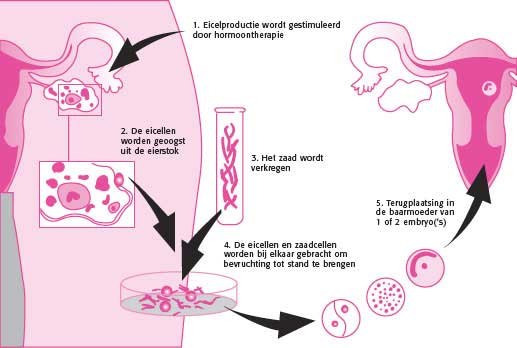
IVM, in vitro maturation, is a variation of IVF which uses all the laboratory components of IVF, but in addition matures eggs in the laboratory. With IVF, a woman undertakes an ovulation induction with gonadotropin medications to make eggs mature in her ovaries before they are harvested from her. With IVM, immature eggs are removed from the ovaries without having to perform an ovulation induction. The eggs are instead matured in the laboratory. They are then fertilized, cultured and transferred as in routine IVF. Injectible medications to stimulate the ovaries are either not used or used in small doses for IVM, which eliminates many side effects for the patient as well as decreasing the expense. IVM also eliminates the need for most of the ultrasound monitoring which is routine for IVF procedures. Blood tests to assess the progress of the ovulation induction are similarly eliminated, making the procedure more convenient and comfortable for the patient.
In the normal menstrual cycle, an egg develops inside of a cyst or follicle over a two week period in response to the gonadotropin hormones FSH and LH that a woman produces. The follicle increases in diameter from about 2 mm to about 20 mm during this time period. During this time, the cells around the egg multiply and produce estrogen. Ultrasound assessments are regularly performed to monitor the growth of the follicle and blood tests are done to monitor estrogen levels and other hormonal assessments. The egg is attached to the follicle wall until increased amounts of the hormone LH (or in medical cycles, HCG) induces enzymes that free the egg from the wall so that it is free floating in the fluid in the follicle. It can then leave the follicle after LH also induces enzymes to create a hole in the follicle wall. During this time, the egg increases very slightly in size and all of the chromosomes are contained in a membrane in the cytoplasm. With the increase in LH as a trigger, this membrane breaks down and the egg divides the chromosomes into two equal groups and moves one of these groups outside the egg (forming a polar body). An egg that has done this is referred to as a mature egg (or MII). Eggs that have not matured, cannot be fertilized to become a baby. In the natural cycle, the egg, which has been freed from the follicle, is then picked up by the end of one of the fallopian tubes. If the egg is lucky enough to be fertilized, it again divides its chromosomes into two equal groups and pushes one of the groups outside the egg to form a second polar body. The remaining chromosomes combine with the chromosomes from the sperm that entered the egg.
In 1935, it was observed that if rabbit eggs were removed from their follicles, some of them would spontaneously mature. In 1965, Edwards (one of the original scientists responsible for the first baby born from IVF) showed that the same thing occurred for human eggs. The first baby born from IVF, Louise Brown, was not born until 1978. The first baby born through IVM was reported in 1991 and came from an egg obtained during a Cesarean section. IVM likely got off to a slow start because of failure to recognize the importance of maintaining the cells surrounding the egg in that egg’s normal development. A commercial media for egg maturation is now available and the details that enable pregnancies to occur at a reasonable rate in appropriately selected patients have also been worked out.
Compared to IVF, the worldwide experience with IVM in humans is limited. Perhaps 10,000 to 20,000 IVM cases using current methodologies have been undertaken in the last decade. By way of comparison, about 60,000 cases of IVF are done in the United States alone each year. There is considerably more experience with IVM in non-human species. IVF had been an important tool in cattle breeding, but was replaced by IVM about ten years ago. More than 100,000 cattle are born utilizing IVM each year.
Most clinical reports suggest that IVM is currently less effective than IVF per case (25-35% clinical pregnancy rate per transfer). For many patients and physicians there are other reasons to prefer IVM to IVF or IVM before IVF in selected patients. For the patient, the process of doing IVM is no more complicated (at times less) than undergoing an ovulation induction with IUI. For self pay patients, the cost is about half the total cost of IVF. For the patients who are the best candidates for IVM, IVM poses significantly less risk for the patient than IVF. IVM also appeals to women who would prefer not to take many medications into their body, but still need to do IVF.
IVM is available throughout the world, but it is considerably less available than IVF. For example, there are about 400 IVF programs in the United States, but the number of programs that offer IVM is likely under twenty. In the United States, IVF cycle reporting is legally mandated, but national reporting views IVM cycles as routine IVF cycles and does not identify programs that offer it. Reporting that does not distinguish IVM from routine IVF cycles, discourages programs from taking on IVM since IVM has a lower pregnancy rate than IVF.
Almost no one recommends IVM for all patients, and the subset of patients, for whom IVM is a good option, is still being defined. Everyone agrees that younger patients with a large number of small follicles (antral follicles) visible in their ovaries on ultrasound are good candidates for IVM. They are also the subgroup of patients who are most likely to get pregnant with IVF.
This introduction to IVM has, perhaps, focused on the reasons a women might not choose to do IVM, namely:
- Doctors are less experienced with IVM than IVF
• It is difficult to find programs that offer IVMa
• There is a lower success rate (per cycle) for IVM than with IVF.
This raises the obvious question of why a woman may choose to do IVM rather than traditional IVF and why an IVF program may choose to develop its ability to offer IVF (which is more complicated than IVF for the laboratory). The answers are all patient centered, namely,
- IVM is vastly easier for the patient to do than traditional IVF (making it an especially good chose for women using a known donor)
• IVM generally costs half as much as IVF (including the cost of medications)
• IVM uses almost no medications; it is based primarily on a woman’s natural cycle
• There are almost no injections of medications required
• There are almost no blood tests required
• There are very few office visits required
• There are few side effects associated with these cycles. The risk of severe ovarian hyperstimulation is eliminated.
Even the success rate of IVF is lesser than the success rate of IVM for example , IVF success rate is depended on the two things like age and which procedure the patient IVF with egg donor or with the sperm donor.
Success Rate |
|
|
IVF fertility treatments |
Chances |
|
IVF with Self eggs |
53% |
|
IVF with donor eggs |
65% |
|
Surrogacy with self eggs |
65% |
|
Surrogacy with donor eggs |
75% |
Now get the brief look to the treatment of the IVF with the most common reason of the fertility is the advanced age.
Success Rate |
|
|
Chances Rate |
Age |
|
52.2% |
35 |
|
47.7% |
35-37 |
|
30.8 % |
38-39 |
|
25.6 % |
40-42 |
|
20 % |
43-44 |
|
10.9 % |
45 |

Devender Gill is an experienced medical blogger & writer on the healthcare researcher with a strong focus on numerous treatments based on the official info from clinics aross network. He Specializes in creating accurate, easy-to-understand medical content covering, medical topics, for instance, IVF, Surrogacy, IUI, ICSI, and other essential ones.
Table of Contents
